INTRODUCTION:
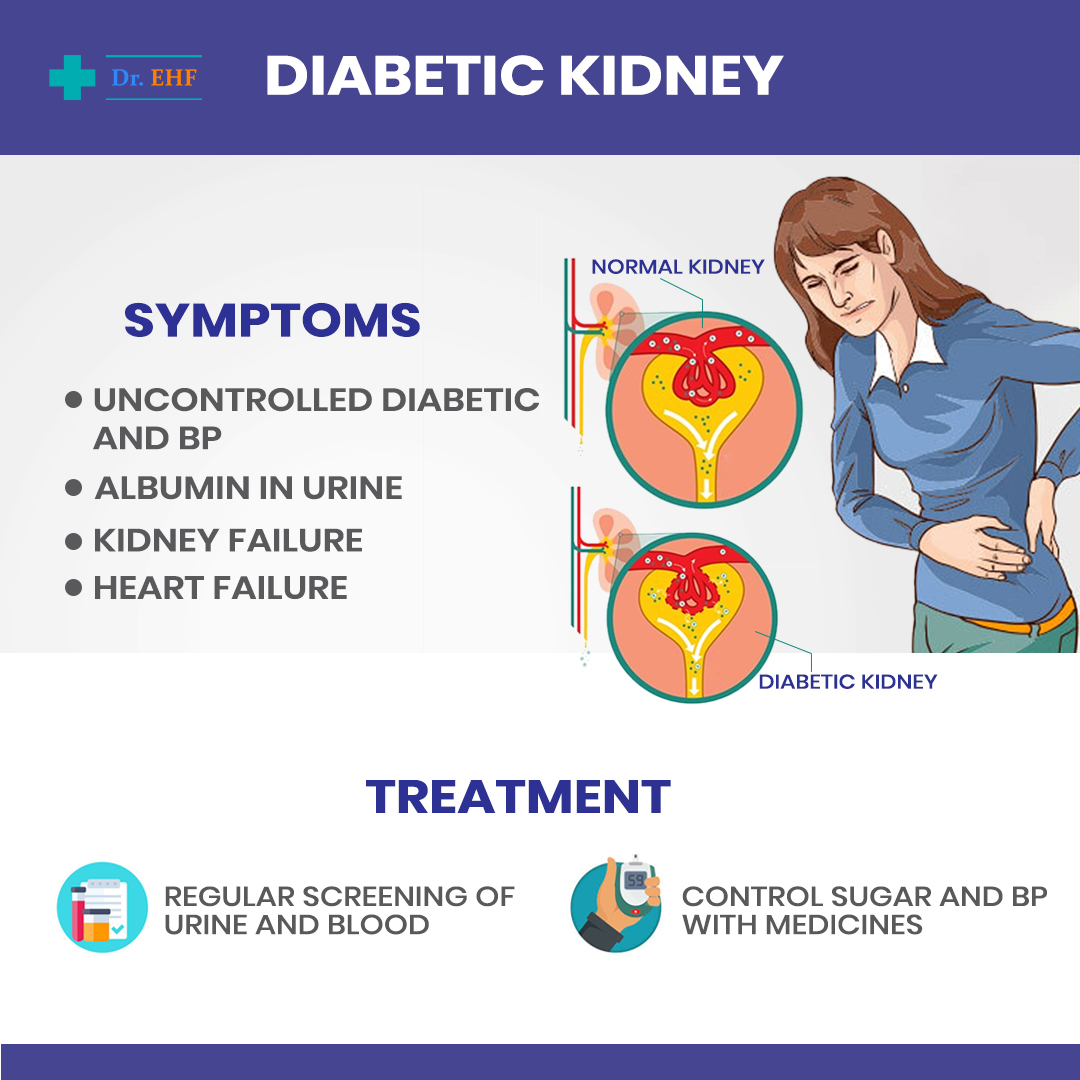
Diabetic Neuropathy OR Diabetic Kidney (DN) is the most common cause leading to Kidney Replacement Treatment globally both in older & even younger patients. Surprisingly it is more common in people with dark skin. When there is presence of albumin in urine, then one can conclude that the kidney is being affected. Albumin in urine gradually increases over the years from a trickle to larger amounts called proteinuria. This also causes BP (Blood Pressure) to rise with serum creatinine finally increasing significantly towards End Stage Renal Disease (ESRD). Early death may also occur if protein loss in urine is not controlled.
Over the last 10 years many scientific studies have shown that control of BP & blood sugar can slow down D N. Therefore, it is very important that diabetic patients can avoid increase of D N, & the sooner the control is started, the lessor will be the chances of having ESRD. This also provides additional protection to the heart.
Prevention of D N starts with early screening of patients for albuminuria & detecting diabetic patients with early signs of nephropathy in both type 1 & type 2 diabetic patients.
Screening diabetic patients is normally the best way to control the spread of D N & strict control of blood sugar is very important to avoid albumin excretion in urine. Early morning urine collection will give the most accurate results & 2 or 3 times reading should be taken so that the average figure will be most accurate.
DOES ALBUMINURIA REFLECT D R? :
No doubt albuminuria can increase a variety of diseases affecting kidney & other organs; however, any other cause of D R should be first excluded. Thorough testing for both urine & blood should be done besides checking for serum creatinine levels also.
SIGNIFICANCE OF ALBUMINURIA:
Presence of both microalbuminuria or proteinuria increases the risk of ESRD & heart disease, especially in diabetic patients. The average life expectancy of diabetic patient on Renal Replacement Therapy (RRT) is 2 years; the main cause of death being heart disease. Younger diabetic patients normally reach end stage disease, but elder patients with affected kidney normally develope heart disease before going to RRT.
PREVENTION OF DIABETIC NEPHROPATHY:
To be able to control D N, screening of patients for retina damage & nerve disease should be done & treated accordingly. Also, firm control of blood sugar levels should be done, because it lowers risk of kidney damage. It was found that reducing BP & load on kidneys, lessens chances of D N. Blood Pressure should ideally be kept below 140/80 to prevent unwanted problems.
Another scientific study found that certain types of BP lowering medicines, called ACE inhibitors, also reduce the progress of kidney damage in such patients. There is another group of medicines called RAS inhibitors which also reduces kidney damage in diabetic patients. These medicines also reduce load on kidneys & hence are able to slow down kidney damage. Potassium levels should also be monitored along with salt intake restrictions. Once patients are stabilized on medicines, reduction of BP is to be maintained to below 130/80 in young adults & below 140/90 in elder diabetic patients. Incase patients BP are not fully controlled, then another medicine can be added.
The effect of sugar control in blood needs to be further studied. Apart from controlled diet, smoking is another risk factor which needs to be stopped.
TARGET:
Hence, we can say that even diabetic patients must have his BP, serum creatinine & urine examination done at least once a year. Suitable medicines need to be taken regularly.
CONCLUSION:
D N is a major cause of patients leading to kidney replacement programme & number of such patients are increasing. Untreated patients are at high risk of kidney & heart disease.
Strict control of blood sugar & BP may reduce further damage to the kidneys. Hence a multidirectional approach is needed to avoid renal disease.
Compiled from various international research journals available at google scholar by D. Mukherjee having 38 years of pharmaceutical (Cardiac, Diabetic, Neurology, Pain & Inflammation products) experience with a Swiss Multinational Company NOVARTIS and edited by Dr Sandeep Ahlawat, MBBS